Hot Watch List (comments).
XNPT (buy)
February 07, 2011 by BiotechInvest
GlaxoSmithKline (NYSE: GSK) and XenoPort, Inc. (Nasdaq: XNPT) announced today that the U.S. Food and Drug Administration (FDA) has accepted for review GSK's response to FDA's Complete Response letter for Horizant(TM) (gabapentin enacarbil) Extended-Release Tablets. Horizant is under review for the treatment of moderate-to-severe primary Restless Legs Syndrome (RLS).
FDA has designated the resubmission as a Class 2 response and set a new Prescription Drug User Fee Act goal date of April 6, 2011.
So, we have 2 months before PDUFA. Is XNPT buy or sell?
"According to the National Institutes of Health, up to 12 million people in the U.S. are afflicted with RLS across a range of severity from mild to severe. The syndrome is characterized by disturbing, unpleasant and sometimes painful sensations in the legs that result in a compelling urge to move. The discomfort is often temporarily relieved by movement. Because symptoms typically occur at night, RLS patients often suffer from sleep disruption. RLS symptoms can be debilitating – published data suggest that RLS can have an impact on quality of life equivalent to, or worse than, major chronic medical disorders such as diabetes and osteoarthritis."
Last time XNPT pps was crashed in Feb. 17, 2010 by FDA CRL:
LONDON & RESEARCH TRIANGLE PARK, N.C. & SANTA CLARA, Calif., Feb 17, 2010 (BUSINESS WIRE) -- GlaxoSmithKline (NYSE:GSK) and XenoPort, Inc. (Nasdaq:XNPT) Wednesday received a Complete Response letter from the U.S. Food and Drug Administration (FDA) regarding the New Drug Application (NDA) for Horizant(TM)(gabapentin enacarbil) Extended-Release Tablets, an investigational non-dopaminergic treatment for moderate-to-severe primary Restless Legs Syndrome (RLS).
A Complete Response letter is issued by the FDA's Center of Drug Evaluation and Research when the review of a file is completed and questions remain that preclude the approval of the NDA in its current form. GSK and XenoPort are currently evaluating the Complete Response letter, in which the FDA indicated that apreclinical finding of pancreatic acinar cell tumors in rats was of sufficient concern to preclude approval of Horizant for RLS at this time. FDA acknowledged that similar findings were known for gabapentin at the time of its approval for refractory epilepsy, but concluded that the seriousness and severity of refractory epilepsy justified the potential risks. The companies are assessing the appropriate next steps and will be communicating with FDA.
GSK submitted its response to questions raised by FDA in a Complete Response letter dated February 17, 2010. GSK's response to FDA included new data from nonclinical studies of Horizant and two epidemiology studies, conducted by GSK, exploring gabapentin use and cancer based on the UK General Practice Research Database.
The resubmission also included a final safety update that provided updated or new safety information on patients in clinical studies who have been treated with Horizant. In order for FDA to be able to consider published gabapentin nonclinical data in their assessment of Horizant, GSK amended the New Drug Application (NDA) for Horizant from a 505(b)(1) to a 505(b)(2) application.
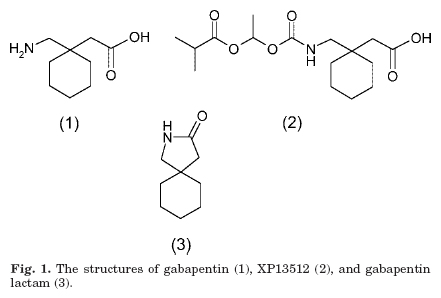
Horizant, also referred to as GSK1838262/XP13512, is a patented new chemical entity. It is an investigational non-dopaminergic treatment for moderate-to-severe primary RLS. It is not approved or marketed anywhere in the world.
So, from today we have 2 months before XNPT PDUFA. And the current pps ($7.64) that is below than OREX pps after CRL (average $8-9). However, pps before CRL was average $19-20.
If FDA approves XNPT NDA for RLS in April 6, 2011 pps will jump at least to $20-25 range i.e. >100% from present price.
What is the probability of approval (or CRL)?
Recently FDA approved Depomed Gralise as a once-daily treatment for post-herpetic neuralgia (PHN).
But Gralise is just a controlled release (CR) form of gabapentin. This extended release allows for the drug to be gradually absorbed into the blood (in upper GI tract over a six to eight hour period), reducing the likelihood of peak concentrations and potentially resulting in fewer side effects than seen with immediate release formulations.
So, FDA approved 1800 mg daily of Gralise (or DM-1796 or gabapentin CR) for PHN.
Is seriousness and severity of PHN justified the potential risks of gabapentin CR approval?
"In the United States each year approximately 1,000,000 individuals develop herpes zoster. Of those individuals approximately 20%, or 200,000 individuals, develop postherpetic neuralgia.
In some cases, treatment of postherpetic neuralgia brings complete pain relief. But most people still experience some pain, and a few don't receive any relief. Although some people must live with postherpetic neuralgia the rest of their lives, most people can expect the condition to gradually disappear on its own within five years."
Is Gralise is a effective cure for PHN?
"The primary endpoint was not achieved with statistical significance for either active treatment regimen, as compared to placebo, over the ten-week treatment period. The mean reductions in average daily pain scores from baseline to end of study were 1.83 (once-daily), 1.72 (twice-daily) and 1.43 (placebo). However, statistical significance relative to placebo was achieved in each of the first six weeks for the once-daily treatment arm and in each of the first five weeks for the twice-daily treatment arm. Pain scores in the placebo group continued to improve in the last four weeks of the study.
The first Phase III PHN trial failed because of a complex trial design and large placebo effect, exactly like the hot flash trials. But a confirmatory, better designed PHN trial succeeded."
Thus, DM-1796 is just a new pain-killer for PHN. And it seems like that DM-1796 is not so strong pain-killer.
Thus, DEPO drug (1800 mg of gabapentin) got FDA approval (in spite of gabapentin induces pancreatic acinar cell tumors in rats and FDA knows it).
But XNPT 1200 mg or 600 mg of XP13512 once per day got CRL because preclinical finding of pancreatic acinar cell tumors in rats.
What is the difference between gabapentin (CR) and XP13512?
DEPO and XNPT were using the different approach to get CR form of gabapentin.
Sustained release formulations of gabapentin have not been successfully developed to date due to the lack of significant colonic absorption of the drug. Poor colonic absorption of gabapentin was confirmed in both rats and monkeys in the this study. Similar results have also been reported following direct administration of gabapentin into the colon of dogs.
In contrast to gabapentin, XP13512 was well absorbed from the colon of both rats and monkeys, consistent with uptake by alternative pathways present in all segments of the intestinal tract. The greatly enhanced colonic absorption of the prodrug suggests that XP13512 is suitable for incorporation into a controlled release formulation.
Depomed designed special formulation with increased retention time in upper GI tract (duodenum). This formulation is patented.
XP13512 is a gabapentin prodrug in CR form. Any way it’s new entity.
So, what is gabapentin cancer story?
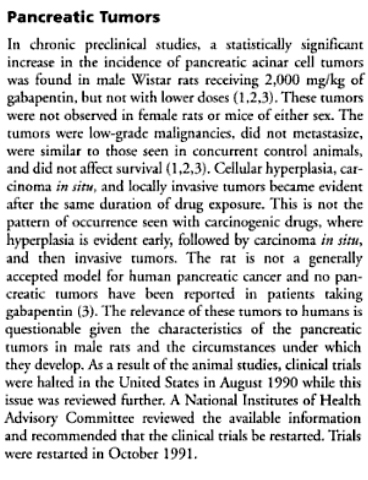
In standard preclinical in vivo lifetime carcinogenicity studies, an unexpectedly high incidence of pancreatic acinar adenocarcinomas was identified in male, but not female, rats.
The clinical significance of this finding is unknown. Clinical experience during gabapentin's premarketing development provides no direct means to assess its potential for inducing tumors in humans.
In clinical studies in adjunctive therapy in epilepsy comprising 2085 patient-years of exposure in patients > 12 years of age, new tumors were reported in 10 patients (2 breast, 3 brain, 2 lung, 1 adrenal, 1 non-Hodgkin's lymphoma, 1 endometrial carcinoma in situ), and preexisting tumors worsened in 11 patients (9 brain, 1 breast, 1 prostate) during or up to 2 years following discontinuation of Neurontin. Without knowledge of the background incidence and recurrence in a similar population not treated with Neurontin, it is impossible to know whether the incidence seen in this cohort is or is not affected by treatment.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Gabapentin was given in the diet to mice at 200, 600, and 2000 mg/kg/day and to rats at 250, 1000, and 2000 mg/kg/day for 2 years. A statistically significant increase in the incidence of pancreatic acinar cell adenomas and carcinomas was found in male rats receiving the high dose; the no-effect dose for the occurrence of carcinomas was 1000 mg/kg/day. Peak plasma concentrations of gabapentin in rats receiving the high dose of 2000 mg/kg were 10 times higher than plasma concentrations in humans receiving 3600 mg per day, and in rats receiving 1000 mg/kg/day peak plasma concentrations were 6.5 times higher than in humans receiving 3600 mg/day.
The pancreatic acinar cell carcinomas did not affect survival, did not metastasize and were not locally invasive. The relevance of this finding to carcinogenic risk in humans is unclear.
Studies designed to investigate the mechanism of gabapentin-induced pancreatic carcinogenesis in rats indicate that gabapentin stimulates DNA synthesis in rat pancreatic acinar cells in vitro and, thus, may be acting as a tumor promoter by enhancing mitogenic activity. It is not known whether gabapentin has the ability to increase cell proliferation in other cell types or in other species, including humans.
Gabapentin did not demonstrate mutagenic or genotoxic potential in three in vitro and four in vivo assays. It was negative in the Ames test and the in vitro HGPRT forward mutation assay in Chinese hamster lung cells; it did not produce significant increases in chromosomal aberrations in the in vitro Chinese hamster lung cell assay; it was negative in the in vivo chromosomal aberration assay and in the in vivo micronucleus test in Chinese hamster bone marrow; it was negative in the in vivo mouse micronucleus assay; and it did not induce unscheduled DNA synthesis in hepatocytes from rats given gabapentin.
No adverse effects on fertility or reproduction were observed in rats at doses up to 2000 mg/kg (approximately 5 times the maximum recommended human dose on a mg/m² basis).
Pregnancy
Pregnancy Category C: Gabapentin has been shown to be fetotoxic in rodents, causing delayed ossification of several bones in the skull, vertebrae, forelimbs, and hindlimbs. These effects occurred when pregnant mice received oral doses of 1000 or 3000 mg/kg/day during the period of organogenesis, or approximately 1 to 4 times the maximum dose of 3600 mg/day given to epileptic patients on a mg/m² basis. The no-effect level was 500 mg/kg/day or approximately ½ of the human dose on a mg/m² basis.
Thus, there was no one pancreatic acinar cell tumors in humans during all these 20 years of using of gabapentin.
One can argues that XNPT XP13512 is not gabapentin. Yes, it’s true. XP13512 is a prodrug of gabapentin.
According this source, FDA was scared by this fact:
"Horizant’s animal studies demonstrated cancerous properties in BOTH female and male rats. Basically, this is a 'red flag' to the FDA, that Horizant has different fundamental, cancer-causing properties than traditional gabapentin."
Thus, XNPT XP13512 is inducing pancreatic cancer in both female and male rats. But FDA think that DEPO gabapentin (CR) is inducing pancreatic cancer only in male rats.
Why "think"?
Because it seems like that FDA never asked DEPO to do 2 years animal study with both female and male rats and dose them by high doses of gabapentin (CR).
Because FDA knows that immediate-release ("IR") gabapentin historically demonstrated pancreatic cancer in a small percentage of male wistar rats when given at extremely high doses for 2 years. No drug induced pancreatic changes were seen in the female rats, or any other species, including humans for the last 20 years. The concentration of gabapentin in rat pancreas were much higher than in human subjects at normal doses.
But DEPO Gralise is not IR but CR form of gabapentin. And XP13512 is also CR form of gabapentin prodrug.
Both drugs have much higher bioavailability and sustained release formulation provide the much longer drug absorption time (Cmax).
May be the reason of pancreatic cancer in both female and male rats is in different form of gabapentin i.e. CR form?
"Formulated with AcuForm delivery technology, DM-1796 is designed for targeted, controlled release to the upper GI tract over a six to eight hour period. This extended release allows for the drug to be gradually absorbed into the blood, reducing the likelihood of peak concentrations and potentially resulting in fewer side effects than seen with immediate release formulations. Greater treatment tolerability and a more convenient dosing regimen made possible with AcuForm could potentially translate into greater patient compliance and ultimately better pain management."
"Unlike gabapentin, XP13512 is well absorbed throughout the intestine, suggesting that it may be successfully incorporated into a controlled release formulation."
"XP13512 is a novel prodrug of gabapentin designed to overcome the pharmacokinetic limitations of gabapentin. In contrast to gabapentin, the prodrug was engineered to be absorbed from all regions of the intestine by high-capacity pathways.
The prodrug was chemically stable and was rapidly converted to gabapentin, presumably by nonspecific esterases present in tissues encountered following oral absorption."
Citations are from published paper.
Since, XP13512 is a new entity XNPT was needed to do 2 years animal study and found that XP13512 induces cancer in both female and male rats. But DEPO drug was just conventional gabapentin (but in CR form) and DEPO knew that FDA will never ask about 2 years animal study for 20 years known drug.
Will FDA approve XNPT Horizant for RLS?
"GSK's response to FDA included new data from nonclinical studies of Horizant and two epidemiology studies, conducted by GSK, exploring gabapentin use and cancer based on the UK General Practice Research Database. The resubmission also included a final safety update that provided updated or new safety information on patients in clinical studies who have been treated with Horizant"
GSK has the results of next study and these results may be were submitted to FDA:
Gabapentin and Risk of Pancreatic Cancer and Renal Cancer (GPRD)
This study has been completed.
High doses of gabapentin are associated with pancreatic acinar cell tumors in rats, but there has been no post marketing pancreatic carcinogenicity signal with gabapentin as reported by spontaneous reports in AERS or in the published literature. In a published case-control screening study of the association of gabapentin with 55 cancers, the only cancer that met the screening criteria for possibly increased cancer risk with gabapentin exposure was renal (including renal pelvis) cancer. This association was judged to be likely due to or substantially accentuated by confounding by cigarette smoking, hypertension, and lifestyle (Cancer Causes Control 2009;20:1821-1835).
The primary objective of this study is to determine whether exposure to gabapentin is associated with an increased risk of developing pancreatic cancer or renal cancer in the United Kingdom (UK) General Practice Research Database (GPRD).
Almost all members of the UK population are registered with a General Practice, which centralizes the medical information not only from the general practitioners themselves but also from specialist referrals and hospital attendances. Over 487 General Practices contribute data to the GPRD.
The study cohort from which cases and controls are drawn is all subjects in the GPRD 1993-2008. Gabapentin was approved in the UK in May 1993. Entry into the study cohort begins Jan 1, 1993 for all those who are registered in GPRD before that time, and at the time of registration if later than Jan 1, 1993. Patients with a first diagnosis of the respective cancer 1995-2008 are risk set matched with up to 10 controls within the same General Practice for age at cohort entry (within two years), sex, and year of entry into the study cohort (within one year). For cases, the index date is the date of first diagnosis of the respective cancer. The index date for controls is set as the date at which the follow-up time from cohort entry is the same as the case. The index date is chosen so as to give the control equal follow-up time to that of the case for ascertainment of use of gabapentin. Cases and controls will be required to have at least 2 years of follow-up in the study cohort before their index date. Data on gabapentin prescriptions are obtained for cases and controls from study cohort entry to the index date.
Crude and adjusted odds ratios and 95% confidence intervals (CI) will be produced from conditional logistic regression models, with additional analyses evaluating for latency and dose-response. For pancreatic cancer, covariates are smoking, body mass index, diabetes, epilepsy, neuropathic pain, and chronic pancreatitis. For renal cancer, covariates are smoking, body mass index, diabetes, hypertension, diuretic use, epilepsy, and neuropathic pain.
Drug: Gabapentin prescriptions
The exposure of interest is gabapentin use as defined by prescriptions recorded by the GPRD general practitioner (British National Formulary codes). Data on prescriptions for gabapentin will be extracted for each case and control from entry into the study cohort up to the index date (the exposure window). Gabapentin exposure will be parameterized as follows: (1) Ever versus never exposed; (2) Number of prescriptions; (3) Duration of exposure; and (4) Cumulative dose. These parameterizations will also be examined with a 2 year lag time from the index date, limiting the exposure window from entry into the study cohort up to 2 years prior to the index date.
Study Population
The study cohort from which cases and controls are drawn is all subjects in the UK GPRD 1993-2008. Entry into the study cohort begins Jan 1, 1993 for all those who are registered in GPRD before that time, and at the time of registration if later than Jan 1, 1993. Follow-up ends Dec 31, 2008, or earlier if the respective cancer is diagnosed, or if the subject leaves the GPRD for any reason including death. There are several advantages to the GPRD dataset for this study. It is a large dataset with detailed longitudinal prescription data, and long term follow-up (mean 7 years) to allow for latency in carcinogenicity. It provides good representation of the elderly who are disproportionately affected by pancreatic and renal cancers, and routinely includes data recorded by general practitioners on potential risk factors such as smoking and body mass index.
Criteria
Inclusion Criteria:
• The study cohort from which cases and controls are drawn is all subjects in the UK GPRD 1993-2008. Entry into the study cohort begins Jan 1, 1993 for all those who are registered in GPRD before that time, and at the time of registration if later than Jan 1, 1993. Follow-up ends Dec 31, 2008, or earlier if the respective cancer is diagnosed, or if the subject leaves the GPRD for any reason including death.
Will be FDA satisfied by these data?
FDA know that rat is not generally accepted model for human pancreatic cancer and no pancreatic tumors have been reported in patients taking gabapentin during last 20 years.
FDA recently approved DEPO Gralise (GABAPENTIN 600MG TABLET; ORAL).
XP13512 were reported as “much improved” or “very much improved” on the CGI-I scale compared to those treated with placebo (78% for 1200 mg XP13512; 45% for placebo; p< 0.0001).
Treatment with 600 mg of XP13512 was also associated with statistically significant improvements in the IRLS and CGI-I endpoints compared to placebo. The unadjusted mean reduction in the IRLS scale score was -13.8 for 600 mg XP13512 patients (p<0.0001 compared to placebo). At the end of treatment, 73% of patients treated with 600 mg of XP13512 were reported as “much improved” or “very much improved” on the CGI-I scale (p<0.0001 compared to placebo).
During the 12-week treatment period, the most commonly reported adverse events for XP13512 were dizziness (24% 1200 mg XP13512; 10% 600 mg XP13512; 5% placebo) and somnolence (18% 1200 mg XP13512; 22% 600 mg XP13512; 2% placebo). These adverse events were generally mild or moderate in intensity.
Withdrawals due to adverse events were 7% in the 1200 mg XP13512 group, 6% in the 600 mg XP13512 group and 6% in the placebo group. There were three reported serious adverse events in the study (one in the placebo group, two in the 600 mg XP13512 group), none of which were considered treatment-related.
It seems like that Horizant 600 mg is effective enough for RLS and it has less side effects than 1200 mg.
Conclusions: the probability of Horizant (600 mg tablet, daily for RLS) is enough high (>70%). FDA should take in consideration the submitted statistics showing that gabapentin was never linked with pancreatic tumors in humans and the facts that rat is not generally accepted animal model for human pancreatic cancer. However, there is some pitfall: FDA can say that XP13512 (prodrug) itself can be more dangerous and carcinogenic than gabapentin.
"Exposure to intact prodrug after dosing XP13512 capsules was low; prodrug Cmax in plasma was approximately 30-fold lower than the corresponding Cmax of gabapentin, and the prodrug was only detected in plasma for the first 4 to 6 h after dosing." cited paper page 328.
Recently FDA approved NVO diabetes drug Victoza. In animal studies, Victoza® caused thyroid tumors—including thyroid cancer—in some rats and mice. It is not known whether Victoza® causes thyroid tumors or a type of thyroid cancer called medullary thyroid cancer (MTC) in people which may be fatal if not detected and treated early.
So, "black box" for Horizant for RLS warning about "pancreatic cancer in rats" is also possible.
Disclosure: I have XNPT positions. High risk, high reward (if keep it through PDUFA).
March 17, 2011 by BiotechInvest
I was temporary in "Short only" mode, however now we have 3 weeks before XNPT binary event. The global market is still unstable because of Japan nuclear power plant uncertainty and the Middle East situation. However, I have decided to buy XNPT today at pps $7. I think it's a good opportunity.
March 28, 2011 by BiotechInvest
I see that biotech investors are very pessimistic about XNPT FDA approval. Well, everybody knows that FDA now is too meticulous about new drug safety. Last XNPT drug already got CRL. Second letter concerning safety will be the final sepulture for Horizant(TM).
What is about just to put similar information in Precautions for Horizant as it was included for Gabapentin (Neurontin)?
Precautions
Carcinogenesis, Mutagenesis, Impairment of Fertility
Gabapentin was given in the diet to mice at 200, 600, and 2000 mg/kg/day and to rats at 250, 1000, and 2000 mg/kg/day for 2 years. A statistically significant increase in the incidence of pancreatic acinar cell adenomas and carcinomas was found in male rats receiving the high dose; the no-effect dose for the occurrence of carcinomas was 1000 mg/kg/day. Peak plasma concentrations of gabapentin in rats receiving the high dose of 2000 mg/kg were 10 times higher than plasma concentrations in humans receiving 3600 mg per day, and in rats receiving 1000 mg/kg/day peak plasma concentrations were 6.5 times higher than in humans receiving 3600 mg/day. The pancreatic acinar cell carcinomas did not affect survival, did not metastasize and were not locally invasive. The relevance of this finding to carcinogenic risk in humans is unclear.
Studies designed to investigate the mechanism of gabapentin-induced pancreatic carcinogenesis in rats indicate that gabapentin stimulates DNA synthesis in rat pancreatic acinar cells in vitro and, thus, may be acting as a tumor promoter by enhancing mitogenic activity. It is not known whether gabapentin has the ability to increase cell proliferation in other cell types or in other species, including humans.
Gabapentin did not demonstrate mutagenic or genotoxic potential in three in vitro and four in vivo assays.It was negative in the Ames test and the in vitro HGPRT forward mutation assay in Chinese hamster lung cells; it did not produce significant increases in chromosomal aberrations in the in vitro Chinese hamster lung cell assay; it was negative in the in vivo chromosomal aberration assay and in the in vivo micronucleus test in Chinese hamster bone marrow; it was negative in the in vivo mouse micronucleus assay; and it did not induce unscheduled DNA synthesis in hepatocytes from rats given gabapentin."
Today XNPT pps is $6.22. The possible losses are at least -50-60% (CRL will be an equivalent to "death penalty" for Horizant). What about the approval upside? XNPT pps before first CRL was $20, so 200% spike after FDA approval now will give pps $18. Enoughfeasible prognosis...
But look at today XNPT options:
Call Options Expire at close Friday, April 15, 2011
Calls
Bid Ask Last Change Vol Op Int
4.0 Call 2.50 2.80 2.62 -0.23 4 409
5.0 Call 1.95 2.10 2.05 -0.09 46 560
6.0 Call 1.55 1.65 1.55 -0.15 3,648 1,076
7.0 Call 1.15 1.25 1.23 -0.02 662 3,698
8.0 Call 0.80 0.95 1.00 0.00 367 2,504
9.0 Call 0.55 0.65 0.65 -0.10 3,231 514
Puts
Bid Ask Last Change Vol Op Int
4.0 Put 0.35 0.45 0.40 0.00 56 1,044
5.0 Put0.85 0.90 0.88 0.08 146 4,684
6.0 Put 1.40 1.50 1.45 0.11 714 868
7.0 Put 1.85 2.10 2.10 0.10 60 550
8.0 Put 2.50 2.75 2.75 0.00 0 9
9.0 Put 3.20 3.50 3.30 0.00 0 22
Obviously that options sellers don't believe that XNPT pps will be $18 after PDUFA at April 6. They are waiting for $3-4 pps.
100 April call contracts 9/0.70 will cost $7k ( and I don't see any feasible put prices to create a "triangle". So I'll just put under the risk $7k. If XNPT win FDA approval the gain will be good enough. Well, CRL will cost me $7k.
It seems like that last CRL did not scared funds, they still hold >90% of XNPT. Strange stubbornness... And they still increase XNPT positions during last 6 months. Do they really believe in FDA approval? Short Interest (% of float as of 03/15/11) was 7.86% i.e. not so many investors think that FDA will send another CRL.
So questions is why XNPT pps is declining during last 2 months? Each day volume was not big, excluding one day when
XenoPort reported that they will stop developing its experimental drugto treat heartburn. This event sent XNPT shares down 12 percent weeks before a U.S. regulator decides the fate of its drug to treat RLS.
May be the funds actually want to accumulate residue 8% of XNPT float before PDUFA? In case of positive FDA decision they will completely dictate XNPT pps and they might drive pps even higher than it was before CRL. It will completely compensate their XNPT losses.
Well, time will tell. Again I will repeat that I think that the probability of Horizant (600 mg tablet, daily for RLS) is enough high (>70%).
But for XNPT I will put under risk no more than 3 % of asset.
It's funny to read next prognosis for XNPT:
"Yee (RBC Capital Markets analyst), who has an "outperform" rating on XenoPort shares, said Horizant has at least a 50 percent chance of getting FDA approval in April. "
I.e. 50:50 case. It's interesting what should do the clients of RBC Capital when they get this 50/50 prediction from analyst? Buy or sell XNPT?
Total Shares Out Standing (millions): 35
Market Capitalization ($ millions): $224
Institutional Ownership: 92.4%
Price (as of 3/25/2011) 6.36
Ownership Analysis # Of Holders Shares
Total Shares Held: 97 32,592,454
New Positions: 17 4,876,497
Increased Positions: 50 8,066,728
Decreased Positions: 27 4,601,779
Holders With Activity: 77 12,668,507
Sold Out Positions: 8 2,185,076
March 30, 2011 by BiotechInvest
Finally I bought 2k shares of XNPT today (already have 100 April 9 calls). I will go through PDUFA with this. Possible losses $13-14k (CRL). Possible gain (approval)...
Good luck!